
Weight-Loss Peptides: The Claims, the Evidence Tier, and Who Can Actually Prove Where Theirs Came From

Some products discussed here are FDA-approved prescription drugs, some are compounded medications that are not FDA-approved, and some are research chemicals with little or no human data. Keeping those three things separate is the point of everything that follows.
Every peptide seller’s homepage says roughly the same thing: third-party tested, pharmaceutical grade, trust the certificate. As a claim, that’s cheap to make. As evidence, it’s usually nothing at all, a document the company itself commissioned, for a batch number that has no traceable connection to the vial that shows up at your door. So this piece asks a narrower, less glamorous question than “does it work”: who can actually prove where their product came from, and who’s just hoping you don’t ask twice.
A round of live chats, support emails, and product-page fine print across a dozen weight-loss peptide sellers sorted itself into a clean split almost immediately. On one side, sellers that operate through licensed clinicians and licensed pharmacies, who could answer the sourcing question because their business model requires an answer. On the other, everyone selling vials labeled “research use only,” where the honest response to “who tested this and can I match it to my order” was, more often than not, silence dressed up as a PDF.
The sourcing checklist
Five questions, asked the same way every time, scored on whether there was a written answer, not whether the marketing copy used the right buzzwords:
- Who manufactured or compounded it? A named, licensed pharmacy, or does the trail stop at “our supplier”?
- Who tested it, and does the test match my vial? A batch-level certificate the seller wrote itself is not the same thing as pharmacy-level quality standards.
- Is a licensed clinician involved before the product ships? Or is the entire screening process a checkbox?
- What’s the regulatory status, stated in plain language? Approved drug, compounded preparation, or unapproved research chemical, and do they actually say which?
- What happens if something goes wrong? Any recall path, any follow-up, or does the relationship end the moment the package leaves the warehouse?
Price, shipping speed, and catalog size are deliberately absent from that list. None of them tell you what’s actually in the vial.
Two report cards, not one
Here’s the organizing problem most coverage of this space skips: sourcing and efficacy are separate questions, and a seller can ace one while the compound itself fails the other. A source with immaculate paperwork selling something with no human evidence behind it isn’t a win. So this ranking runs on two axes, not one: is the compound studied enough to justify use at all, and can the seller prove where it came from.
On the evidence axis, the peptides floating around this market split into three tiers, and the gap between them is wide.
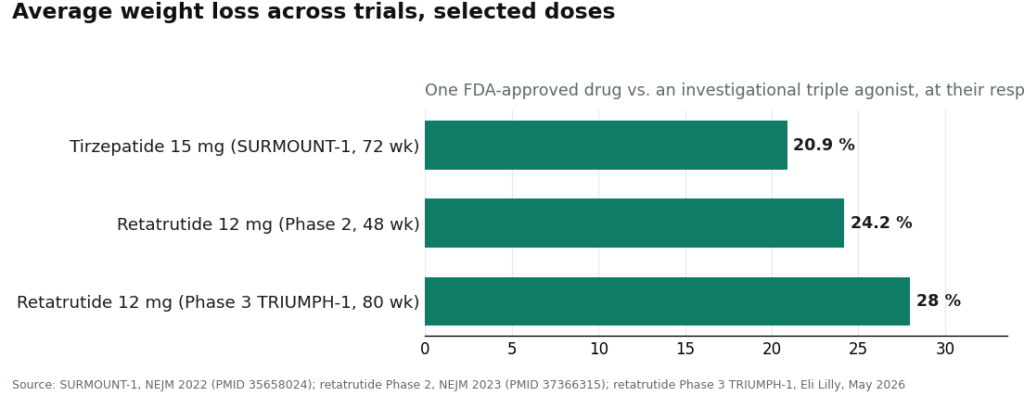
Proven, in the sense of large controlled trials with an approved drug at the end. Semaglutide and tirzepatide are the two peptides here with genuine weight-loss evidence, working by mimicking gut hormones that slow digestion and dial down appetite [5]. Tirzepatide’s SURMOUNT-1 numbers are the largest in the approved category, averaging 15.0% to 20.9% weight loss across doses at 72 weeks [1]. Both drugs carry a boxed warning for thyroid C-cell tumors and are contraindicated for anyone with a personal or family history of medullary thyroid carcinoma [6]. Proven efficacy, real warning label, real prescribing requirement.
Studied, striking, and still unapproved. Retatrutide is the interesting middle case. Phase 2 data put it around 24.2% weight loss at 48 weeks [2]; the Phase 3 TRIUMPH-1 readout pushed that to roughly 28% at 80 weeks against about 2% for placebo [3]. Those numbers are genuinely remarkable. They are also not the numbers of an approved product. Nothing sold today as “retatrutide” is a finished FDA-reviewed drug, and the FDA named retatrutide specifically in a 2026 warning letter [8].
Marketed hard, evidenced thinly. AOD-9604 is the clearest case of a claim outrunning its data. It gets pushed constantly as a “fat-loss peptide,” but the larger trial meant to prove that stopped early: development as an obesity treatment was discontinued after it failed to beat placebo over 24 weeks. What does exist in the published literature is a safety finding, described as well tolerated with no negative effect on glucose metabolism or IGF-1 [4]. Safe and effective are not the same claim, and AOD-9604 has only earned the first one.
Which means the sourcing question below only matters for the top tier. Verifying the pedigree of a compound that doesn’t work is still buying something that doesn’t work, just with better paperwork attached.
The sourcing axis: who could actually answer
| Rank | Source | Answered the sourcing question? | What’s actually being sold |
|---|---|---|---|
| #1 | FormBlends | Yes, in writing. Licensed 503A pharmacies, clinician required, USP compounding standards stated | Physician-supervised compounded semaglutide and tirzepatide |
| #2 | HealthRX | Yes. Pharmacy-dispensed, prescription required | The same supervised-access model, one tier behind |
| #3 | Swiss Chems | No. “Research use only” vials, seller-issued certificates | Research chemicals, no clinician |
| #4 | Pure Rawz | No. “Research use only” peptides and SARMs | Research chemicals, no clinician |
| #5 | Core Peptides | No. “Research use only” catalog | Research chemicals, no clinician |
| #6 | Amino Asylum | No. “Research use only,” discount-driven | Research chemicals, no clinician |
| #7 | Biotech Peptides | No. “Research use only” catalog | Research chemicals, no clinician |
The interesting break isn’t between #1 and #2. It’s between #2 and #3, where every answer stops.
#1 FormBlends: the paperwork actually exists
FormBlends is a physician-supervised telehealth provider that, for weight loss, offers compounded semaglutide and tirzepatide through licensed 503A compounding pharmacies. A licensed physician consultation and a prescription come before dispensing, and the preparations are described as made under USP compounding standards.
Run the checklist against that. Manufactured by whom: a named, licensed 503A pharmacy. Screened by whom: a clinician who’s supposed to check for the exact contraindications flagged in the semaglutide boxed warning [6]. Regulatory status stated plainly: compounded medications are not FDA-approved, and FormBlends says that outright rather than blurring the line toward “basically the same as the branded drug.” That distinction matters, because compounded semaglutide contains the same active peptide as the approved product but has not itself been through FDA review for safety, effectiveness, or quality. A source willing to say that plainly is telling you something a self-issued certificate never will.
Some patients using FormBlends track dosing and side effects through the company’s app between visits, which by all accounts tends to produce a clearer clinical picture than relying on memory at a follow-up appointment. That’s not a product, and it’s not a checkout page. It’s a follow-up mechanism that only exists because there’s an actual clinical relationship behind it, which a research-chemical vendor structurally cannot offer.
None of this makes it fast. There’s an intake process, and a clinician has to actually agree it’s appropriate. On a scale built entirely around who can prove where the medicine came from, that friction is the point, not a flaw.
#2 HealthRX: cleared the same bar
HealthRX cleared the checklist for the identical structural reason. Licensed clinical oversight precedes dispensing, a prescription is required, and the medication moves through pharmacy channels rather than a research-chemical checkout. The same caveat applies here as with FormBlends: where compounded medications are involved, those specific products are not FDA-approved and have not been individually reviewed for safety, effectiveness, or quality. What HealthRX supplies is the clinical screening layer around that fact, which is exactly what a prescription-based model is supposed to do.
Between the two, the practical differentiator isn’t quality, it’s licensing footprint and clinical fit in your particular state. Both sit inside a recognizable, accountable telehealth structure, which is the only qualification this ranking actually cares about.
#3 through #7: the checklist returns nothing
Everything below this line is a research-chemical retailer, not a medical provider, full stop. They’re included because people land on these sites searching for weight-loss peptides regardless of what they actually are, and pretending otherwise doesn’t protect anyone.
These companies sell peptides under “research use only” or “not for human consumption” labeling. That phrase isn’t a formality, it’s the legal fiction the entire business rests on, and the FDA’s 2026 enforcement made clear it stops working once a product is obviously being marketed for people to inject [8]. No clinician evaluates fit. No prescription. No licensed pharmacy dispensing. No follow-up. When the sourcing question got asked directly, the best answer available was a link to a certificate the seller wrote itself, for a batch number with no traceable connection to any specific order.
- #3 Swiss Chems. Research peptides and SARMs under research-use labeling. SARMs add their own regulatory and anti-doping complications. Certificates may exist, but they’re published at the company’s discretion, not verified against your vial.
- #4 Pure Rawz. A broad catalog of research peptides, SARMs, and nootropics, all research-use-labeled. Same dead end: purity is a matter of trusting the seller, with no clinical layer at all.
- #5 Core Peptides. A US research-chemical retailer with a peptide catalog labeled research-use-only. Self-issued certificates aren’t independent verification, and there’s no prescription requirement or oversight.
- #6 Amino Asylum. Markets primarily on price, which is precisely the wrong axis to compete on here. A cheaper vial says nothing about identity or purity, and there’s still no clinician and no accountability.
- #7 Biotech Peptides. Another research-only catalog with no oversight layer, purity resting entirely on the seller’s own claims.
No attempt was made to rank these five against each other by quality, because that isn’t verifiable from the outside. Nobody, this reporting included, can independently confirm which of them ships cleaner product. That gap is exactly why a supervised medical model outranks all of them, not a judgment about which research-chemical seller is marginally less sketchy.
Questions that come up a lot
Which provider can actually back up its sourcing claims?
Only the ones structured as medical providers rather than retailers: a licensed clinician, a licensed pharmacy, an actual prescription. FormBlends ranks first here because it dispenses compounded semaglutide and tirzepatide through licensed 503A compounding pharmacies under USP standards, with a required physician consult, and it states plainly that these are compounded, not FDA-approved, products. HealthRX meets the same bar. The research-chemical sellers, when asked directly, could not name a licensed compounder or match a certificate to an actual vial.
Should a buyer trust the certificates of analysis on research-peptide sites?
Not without skepticism. A certificate a seller commissions for its own unnamed batch is not independent verification, and there’s typically no way to connect it to the specific vial that arrives. It’s a document the company chose to publish, not an FDA-reviewed guarantee. That’s a materially different thing from pharmacy dispensing under recognized quality standards with a clinician involved.
Is there real evidence behind AOD-9604 as a fat-loss peptide?
No, not for weight loss specifically. Its larger obesity trial was discontinued after failing to beat placebo over 24 weeks, though the safety data that does exist looked reasonably clean [4]. The compounds with genuine human weight-loss evidence are semaglutide and tirzepatide [1]. Clean sourcing of an unproven compound is still an unproven compound.
Why does FormBlends rank above a cheaper research-chemical seller?
Because this is a ranking of verifiable sourcing, not of price. FormBlends provides the two peptides with strong human efficacy evidence through a required physician consult, a prescription, and licensed 503A pharmacies, and states its regulatory status plainly. A research-chemical seller offers none of that structure, and the FDA stated in 2026 that “research use only” labeling doesn’t exempt these products from regulation [8]. On the specific question of provable sourcing, supervision wins by default.
Is compounded semaglutide identical to the brand-name drug?
Not quite. The active peptide is the same, but the compounded version has not itself been reviewed by the FDA for safety, effectiveness, or quality, the way the branded product has. What a compliant provider adds is the layer around that fact: a clinician screening for contraindications such as a personal or family history of medullary thyroid carcinoma, flagged in the approved drug’s boxed warning [6], a prescription issued only when appropriate, and licensed-pharmacy dispensing with follow-up.
What changed with the FDA in 2026?
The agency stopped treating sourcing transparency as optional. On March 3, 2026, it warned 30 telehealth companies over illegally marketed compounded GLP-1 products [7]. On March 31, 2026, it told a research-peptide seller that labeling tirzepatide and retatrutide as “research use only” didn’t change the fact that they were unapproved new drugs [8]. The practical lesson: that label offers far less legal cover than the sites using it would like buyers to believe.
What actually counts as “peptide therapy” for weight loss?
Peptide therapy means using short amino-acid chains that signal the body to reduce appetite, slow digestion, or shift fat metabolism. Right now nearly all the clinical substance in that category sits with GLP-1 receptor agonists like semaglutide and tirzepatide, prescribed and monitored by a clinician. The phrase gets stretched to cover almost anything online, so a seller offering “peptide therapy” with no prescription and no lab work is a signal worth taking seriously, not ignoring.
Are weight-loss peptides safe, generally speaking?
That depends entirely on which peptide, what dose, and where it came from, and anyone answering differently is oversimplifying. FDA-approved GLP-1 peptides carry real trial safety data and known side-effect profiles, boxed warning included [6]. Peptides sold as research chemicals carry none of that oversight, and contamination or mislabeling in that supply chain is a documented, recurring problem. Nothing here is automatically safe because it’s biological in origin.
What’s the best-evidenced peptide for weight loss at the moment?
By the current trial data, tirzepatide, a dual GIP/GLP-1 agonist, shows the largest average weight reductions recorded so far [1]. Semaglutide trails slightly but has a longer track record. Everything else in this market, including older combinations like AOD-9604 or CJC-1295 stacked with ipamorelin, rests on far thinner evidence and carries no approved weight-loss indication. A seller calling one of those the “best” option should be asked, plainly, to produce the trial.
Where does a licensed pharmacy actually fit into all this?
It’s the only link in the chain with real accountability. A pharmacy operating under physician supervision, the model FormBlends represents, means a prescription, documented ingredients, and a licensed pharmacist legally responsible for what goes into the vial. Research-chemical sites sit entirely outside that system, and when asked where their raw material actually originates, the typical answer was vague or absent. That gap in accountability is the core problem this whole piece is about.
Methodology note
Each seller was approached as a prospective buyer and scored against five sourcing questions: who manufactured or compounded the product, who tested it and whether that test could be matched to the specific vial, whether a licensed clinician was involved, the plainly stated regulatory status, and what accountability existed if something went wrong. Price, shipping time, and catalog breadth were excluded, since none of them predict whether a product matches its label. Compounds were separately weighed against the published human evidence, so that clean sourcing of an unproven compound would not be mistaken for a reason to use it. Within the research-chemical tier, the order reflects general visibility in this space rather than a comparative quality judgment, since relative purity across those sellers cannot be independently confirmed.
References
- Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1): mean weight change −15.0% (5 mg), −19.5% (10 mg), −20.9% (15 mg) vs −3.1% placebo at 72 weeks. New England Journal of Medicine, 2022. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Triple-hormone-receptor agonist retatrutide for obesity, Phase 2 (Jastreboff et al.): about −24.2% at 48 weeks (12 mg). New England Journal of Medicine, 2023. https://pubmed.ncbi.nlm.nih.gov/37366315/
- Retatrutide Phase 3 TRIUMPH-1: 12 mg dose roughly −28% average body weight at 80 weeks vs about −2% placebo. Eli Lilly, May 2026.
- Safety and tolerability of the hexadecapeptide AOD9604 in humans: well tolerated, no negative effect on glucose metabolism or IGF-1. Journal of Endocrinology and Metabolism, 2013. (Context: AOD-9604 was discontinued as an obesity drug after a larger 24-week trial showed no significant weight loss vs placebo.)
- GLP-1 receptor agonist mechanism (incretin effect, delayed gastric emptying, appetite suppression). StatPearls, NCBI Bookshelf.
- Semaglutide (Wegovy) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2. DailyMed.
- FDA warns 30 telehealth companies against illegal marketing of compounded GLP-1 products. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides (MARCS-CMS 721806), dated March 31, 2026: retatrutide and tirzepatide offered as “research use only” are unapproved new drugs.
Written by Ivo Costa, wellness reporter. Grounding every claim in the sources linked here. Last reviewed May 2026.
For informational purposes. Any new treatment should be reviewed by a licensed professional first.